YO Clinic October 2021

Ayşe Yildiz Tas M.D. Febo. – Clinical Researcher Ophthalmologist at Koc University, School of Medicine, Department of Ophthalmology, Istanbul, Turkey

Murat Hasanreisoglu M.D. FEBO, Assoc. Prof. – Clinical Researcher Ophthalmologist at Koc University, School of Medicine, Department of Ophthalmology, Istanbul, Turkey
Paediatric uveitis accounts for 5–10% of all uveitis and differs from adult uveitis in that it can be asymptomatic and become chronic and cause damage to ocular tissues. Major challenges in paediatric uveitis groups are variations in clinical presentation, difficulties in ocular examination, extended burden of the inflammation over quality of life, limited treatment modalities and risk of amblyopia. There are also unique forms of uveitis and masquerade syndromes in childhood, while some entities commonly encountered in adults are rare in children. In addition, the side effects of therapies such as retarded growth and development can affect the child and may present a burden to the child’s family. Close follow up is also necessary because of a possibility of asymptomatic vision threatening clinic and uveitis flare ups during immunomodulatory therapy.
The International Uveitis Study Group (IUSG) and Standardization of Uveitis Nomenclature (SUN) criteria allow ophthalmologists to classify uveitis for research and clinical purposes. These criteria define the anatomical location, onset, duration, and the course of disease and aid in the monitoring of disease activity in children with uveitis. (Table 1)
Table 1: Anterior, intermediate, posterior, and panuveitis in children.
| Anatomical classification of uveitis | Common causes |
| Anterior uveitis | Non-differentiated anterior uveitisJuvenile idiopathic uveitisJuvenile ankylosing spondylitisJuvenile psoriatic arthritisJuvenile reactive arthritisSarcoidosisBlau syndromeTubulointerstitial nephritis and uveitisKawasaki syndromeInflammatory bowel diseaseHerpetic anterior uveitisTraumaForeign body |
| Intermediate uveitis | Pars planitisSarcoidosisAnkylosing spondylitisLyme diseaseTuberculosisMultiple sclerosis |
| Posterior uveitis | UndifferentiatedToxoplasmosisToxocariasisSarcoidosisEales disease |
| Panuveitis | UndifferentiatedBehcet diseaseSarcoidosisToxoplasmosisVogt-Koyanagi -HaradaTuberculosis |
- Epidemiology and demographics
Childhood uveitis accounts for 5–10% of all types of uveitis. The incidence and prevalence of the disease varies in different countries and populations. In the United Kingdom, the annual incidence of pediatric uveitis is 5 per 100,000 children. Pediatric uveitis has been found to be more common in girls, like other autoimmune conditions. Most uveitides in children are idiopathic; however, the most common identifiable cause of uveitis in children is juvenile idiopathic arthritis (JIA). Uveitis is most frequently associated with oligoarticular and rheumatoid factor negative polyarticular categories of JIA. Among infectious causes of uveitis in children, toxoplasmosis is the most common etiology.
- Anterior Uveitis
Anterior uveitis includes inflammation of the iris, the anterior part of the ciliary body or both (iridocyclitis). In the pediatric population, anterior uveitis is the most common form of uveitis and includes 44%–52% of all pediatric cases.
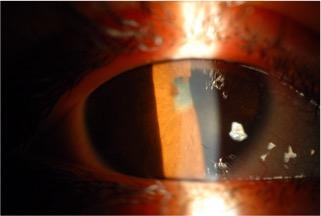
JIA-associated anterior uveitis usually presents as a chronic non-granulomatous uveitis and it is the most common identifiable cause of childhood uveitis. The prevalence of JIA related uveitis is higher in Caucasian compared to African-American children. There are three major types of JIA: systemic, oligoarticular arthritis, and polyarticular arthritis. Patients with JIA may first present with uveitis in 3–7% of cases, but they are usually asymptomatic. The major risk factors for severe uveitis complications are a short time interval from the onset of arthritis to the onset of uveitis, male gender, a young age at onset of uveitis and synechiae at presentation (Figure 1). Uveitis activity declines around age 9 and peaks later in adolescence.
Figure 1: Seclusion of the pupil, pupillary membrane and cataract in a child with JIA-associated anterior uveitis.
Juvenil Seronegatif spondyloarthropathies (JSpA) includes psoriatic arthritis, ankylosing spondylitis, enthesitis related arthritis (ERA), reactive arthritis, and enteropathic arthritis. Defining characteristics of JSpA are enthesitis and axial arthritis. Uveitis occurs in one-quarter of children with JSpA, like the incidence in adult-onset disease.
Tubulointerestitial nephritis and uveitis (TINU) is often diagnosed based on the presence of systemic symptoms, including fever, weight loss, abdominal and flank pain, and arthralgia associated with renal dysfunction evidenced by increasing urea and creatinine levels, proteinuria, microhematuria and glycosuria. An elevated urinary beta-2-microglobulin level has been reported as a very helpful laboratory marker. The median age of onset is 15 years, and the condition is more commonly seen in females. The uveitis is mostly acute bilateral anterior uveitis often with pain and photophobia; however, posterior (vitritis, papillitis, cystoid macular edema, chorioretinitis, and multifocal choroiditis) or intermediate uveitis can occur as well.
Herpetic anterior uveitis. Infectious etiologies make up to 13% of all childhood uveitis. Type 1 and 2 herpes simplex virus (HSV) and varicella zoster virus (VZV) can present as acute unilateral granulomatous or non-granulomatous anterior uveitis. It is important to diagnose these cases early since delayed diagnosis can result in significant vision loss. The treatment required for infectious etiologies is different from the treatment in autoimmune uveitis. Prophylactic treatment is often needed.
- Intermediate uveitis
Intermediate uveitis is typically the inflammation of the vitreous body and peripheral retina. The idiopathic form of intermediate is called pars planitis; however, sarcoidosis and juvenile multiple sclerosis may be causes of intermediate uveitis in up to 10% of pediatric patients.
Pars planitis is a diagnosis of exclusion. It is the cause of 5%–26.7% of all pediatric uveitis. Mild anterior uveitis with small keratic precipitates can be seen in up to 50% of patients. Neovascularization of the optic disc or associated with snowbanks may cause vitreous hemorrhage and is more common in children than adults with pars planitis. Cystoid macular edema is a common complication occurring in 12–50% of children and can be accompanied by peripheral retinal vasculitis. Snowballs are round yellowish-white aggregates of inflammatory cells in the vitreous that lie close to the retina (Figure 2). Dense vitreous condensation may cause leukocoria, sometimes mistaken for cataracts. The severity of the disease and the complications of pediatric pars planitis are higher in patients younger than 7 years.
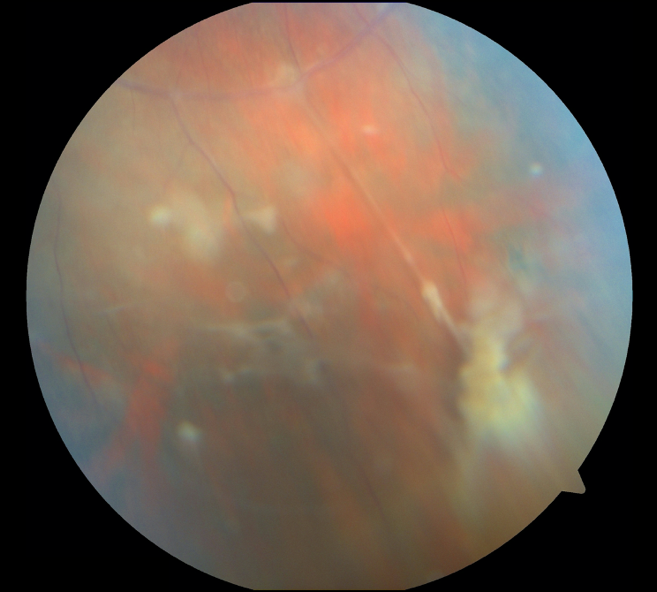
Figure 2: Snowball opacities and vascular sheathing in a child with pars planitis.
Less frequently, ocular sarcoidosis, Lyme disease, multiple sclerosis, and tuberculosis in underdeveloped countries can cause intermediate uveitis.
- Posterior and Panuveitis
Both, posterior and panuveitis, can be infectious or non-infectious. The involvement may predominantly be in the choroid (e.g., birdshot chorioretinopathy) or predominantly in the retina and secondarily affect the choroid (e.g., toxoplasmosis).
Toxoplasmosis is one of the most common causes of posterior uveitis in children. The hallmark of an active Toxoplasma lesion is focal necrotizing retinochoroiditis with focal vitritis. It appears as a ‘headlight in the fog’ on dilated funduscopy. The anterior chamber might be secondarily involved in severe inflammation and manifests with granulomatous anterior uveitis and high intraocular pressure. The diagnosis of toxoplasmosis is mostly clinical, but the parasite DNA may be detected on PCR of the aqueous or vitreous humor.
Toxocariasis is a parasitic infection. Ingestion or exposure to T. canis, and less commonly T. cati, larvae can cause systemic infection. Toxocara uveitis, especially in children between the ages of 2 and 9, can present with posterior pole granuloma, peripheral granuloma, and diffuse vitritis.
Vogt-Koyanagi-Harada Disease is more common in people with greater skin pigmentation. Pediatric VKH is relatively uncommon and has 4 stages: prodromal, acute uveitic, convalescent, and chronic. The prodromal stage is characterized by flu-like symptoms with neurological and auditory manifestations. The uveitic stage typically consists of bilateral panuveitis with thickening of the choroid and disc swelling, multiple exudative retinal detachments, and mild-to-moderate vitritis. At this stage, granulomatous anterior uveitis with iris nodules can occur. Recurrent and prolonged inflammation is common in children and can trigger potentially blinding complications like subretinal fibrosis, choroidal neovascularization, posterior synechiae, cataract, and glaucoma. In the convalescent phase, there is a tendency for the disease to become chronic, with the occurrence of pigmentary changes in the fundus that result in a ‘sunset-glow’ appearance with foci of hyperpigmentation and Daleén-Fuchs like nodules appearance in the midperiphery. The chronic stage manifests with a recurrent, mainly granulomatous, anterior uveitis.
Behçet uveitis. The principal pathological process in Behçet’s disease is a vasculitis predominantly involving the veins and is characterized by oral ulceration, genital ulcers, skin lesions, ocular lesions, gastrointestinal involvement, vascular lesions, and neurological manifestations. Incidence of ocular manifestations in children is less common compared with adults. The mean age at onset of pediatric Behçet is in late childhood (10-15 years). Pediatric patients typically fulfill the diagnostic criteria for Behçet disease after the age of 16. Pediatric Behçet uveitis is more frequently found in males and ocular involvement is bilateral in 80% of the cases. Ocular involvement in Behçet’s disease is characterized by recurrent, but spontaneously resolving, attacks of hypopyon iridocyclitis with or without panuveitis. Visual prognosis is variable in pediatric cases; however, it is typically better than adults. Cataract, glaucoma, macular edema or maculopathy, and optic atrophy are the most common complications.
- Masquerade syndromes
Masquerade syndromes should be considered in the differential diagnoses of pediatric patients with uveitis, especially in cases with incomplete and less favorable response to typical anti-inflammatory therapy. The most common masquerade syndromes in this age population include retinoblastoma, leukemia, medulloepithelioma, xanthogranuloma, retinitis pigmentosa, retinal detachment and intraocular foreign body. Leukemia is the most common masquerade syndrome in this age group and presents with signs including cotton-wool spots, retinal hemorrhage, vascular sheathing, and perivascular exudates.
- Management: General Principles
Systemic medications such as corticosteroids have deleterious side effects on bone development and growth of children and should be used judiciously employed. Similarly, steroid-sparing immunosuppressives should be used with close monitoring of the patients. Outcome of the surgical procedures in management of various complications of pediatric uveitis, such as cataract, retinal detachment, glaucoma, are often frustrating and disappointing. Thus, prevention and early identification and treatment of any vision threatening complications plays the most important role in the management of pediatric uveitis.